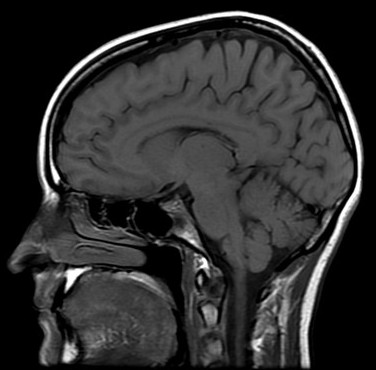
Useful
for detailed assessment of the midline structures including corpus
callosum, sella and suprasellar structures, clivus, craniocervical
junction, as well as the bone marrow.
Normal
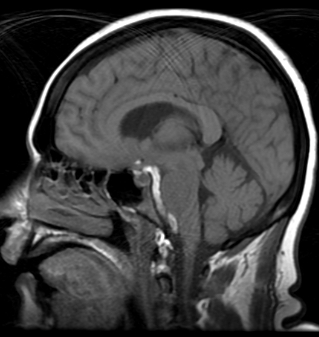
Hyperintense
signal abnormality in the posterior aspect of the corpus callosum (lipoma).
Also, there is an optic tract glioma
Hyperintense
signal anterior to the pons representing prepontin acute hemorrhage
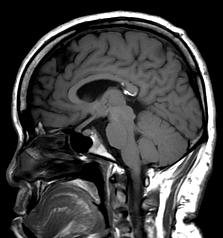
Sagittal T1
sequence showing empty sella
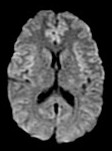
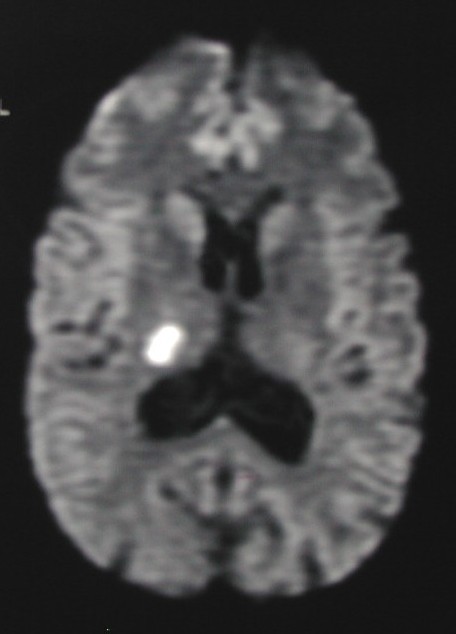
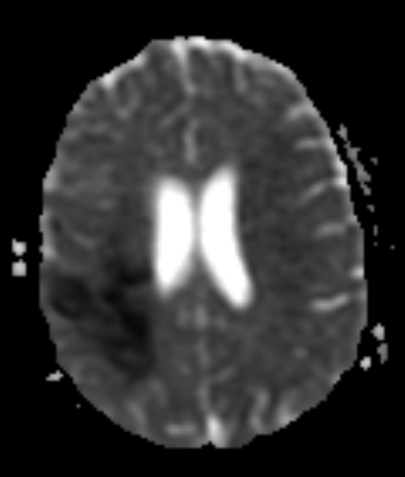
2- Axial DW:
Particularly
useful to determine if there is acute or subacute infarct. Its
sensitivity is quite high, while the specificity is limited and requires
clinical correlation.
Normal
Acute small thalamic infarct
(right).
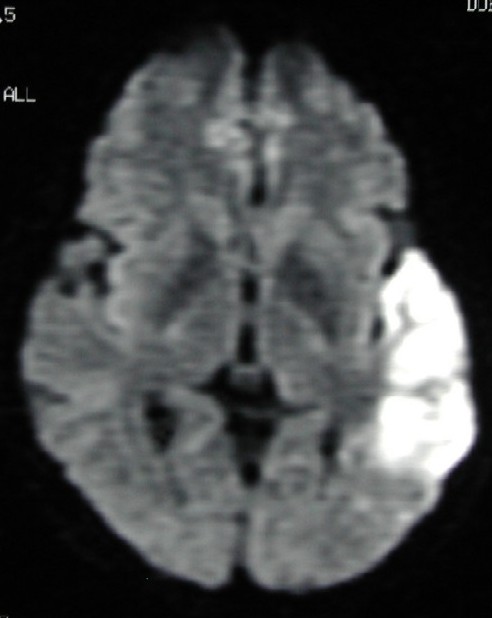
Acute
temporoparietoccipital infact (left)
Menengioma(m)
in the anterior left middle cranial fossa - also demonstrates
hyperintensity
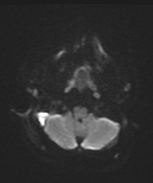
Epidural
abscess adjacent to the right mastoid (secondary to mastoiditis)
demonstrating hyperientensity
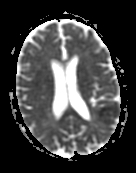
3- Axial EP
Predominantly
useful to determine if the hyperintensity on DF scan is due to infact or
artifactual ("T2 shine-through phenomenon".
Normal
Hypointense
area in the left parietal area is due to acute infact
Acute
infarct in the right parietal area
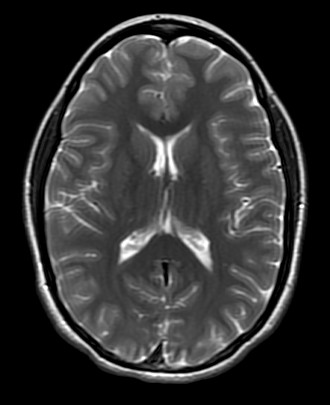
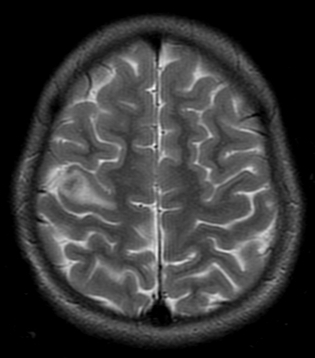
4- Axial T2 spin
echo (SE)
Axial T2 SE is
considered a gold standard to assess the brain anatomy, as well as
paranasal sinuses and temporal bone aeration.
Normal
Periventricular
leukomalacia: clearly demonstrated using axial T2 images.
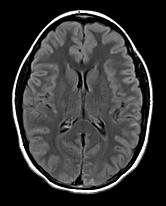
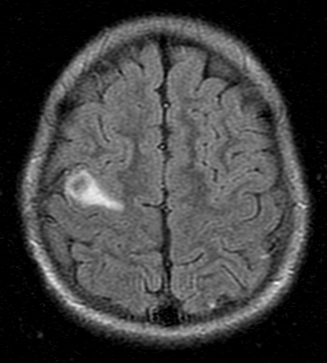
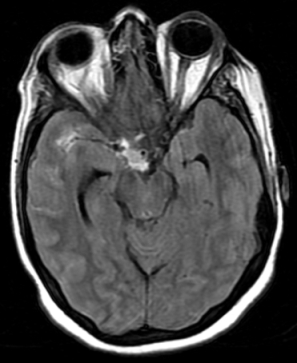
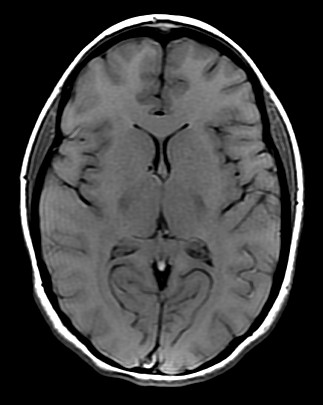
5- Axial Flair
Flair is a
good supplement to T2 to assess the white matter conditions and generally
more sensitive than T2. Flair is also quite sensitive to
determine if there is subarachnoid hemorrhage.
Normal
Intracranial
tuberculosis is clearly more conspicuous on flair (1st: T2, 2nd:
flair).
Acute
subarachnoid hemorrhage
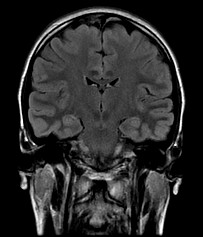
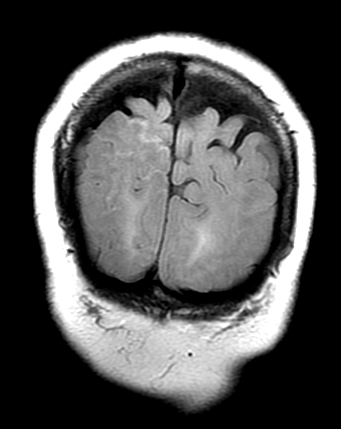
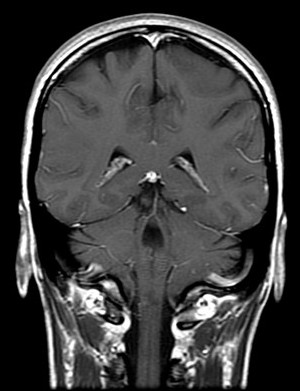
6- Coronal Flair
Coronal Flair
is a good supplement to axial flair, to confirm the signal abnormalities
seen on axial scans, as well as for further assessment of the temporal lobes.
Normal
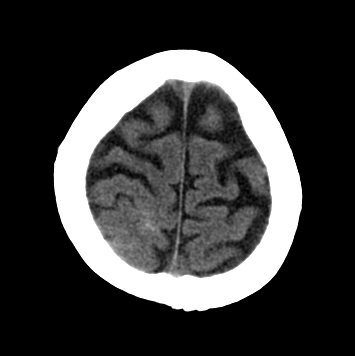
Subtle subarachnoid
hemorrhage on CT and on Flair coronal scan as a hyperintense sulci.
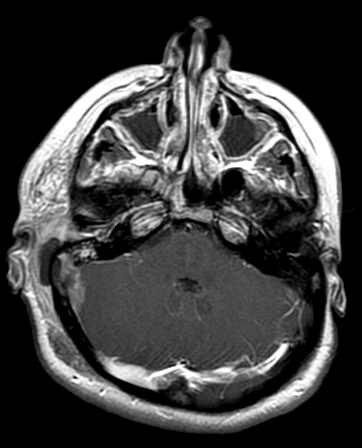
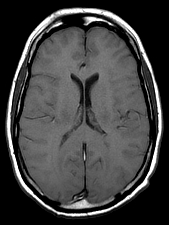
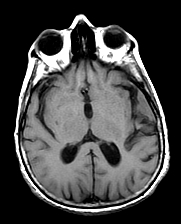
7- Axial pre-contrast T1
spin echo (SE)
Main purpose
of this sequence is to establish a baseline for the post contrast scan.
Also, T1 spin echo can be useful to assess intracranial hemorrhage as
well as fat containing lesions.
Normal.
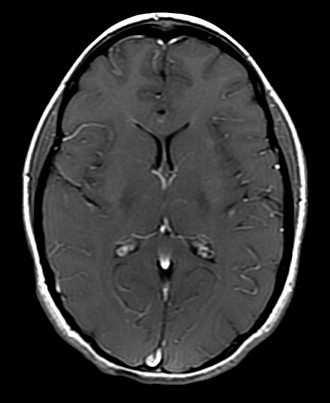
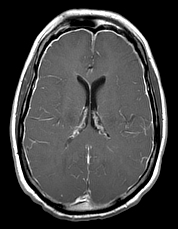
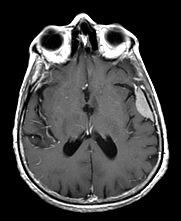
8- Axial post-contrast
T1 spin echo (SE)
Axial
post-contrast scanning is a gold standard to rule out enhancing
intracranial lesions and also to assess the enhancement pattern of a known
lesion.
Normal
Epidural abscess
secondary due mastoiditis (left side) demonstrating intense contrast
enhancement (same patient - see DW scan above). Also see sinusitis.
Precontrast scan is
normal. However, post contrast scan demonstrates intense diffuse menengial
enhancement (Intracranial hypotension).
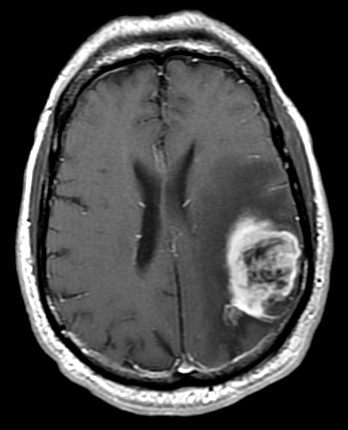
Glioblastoma
Multiforme (GBM)
Left temporal area
menengioma is not noticeable on pre-contrast T1 (first image) while it is
easily noticeable on post-contrast scan (second image). Post-contrast scan
is important to assess the extent of the tumor
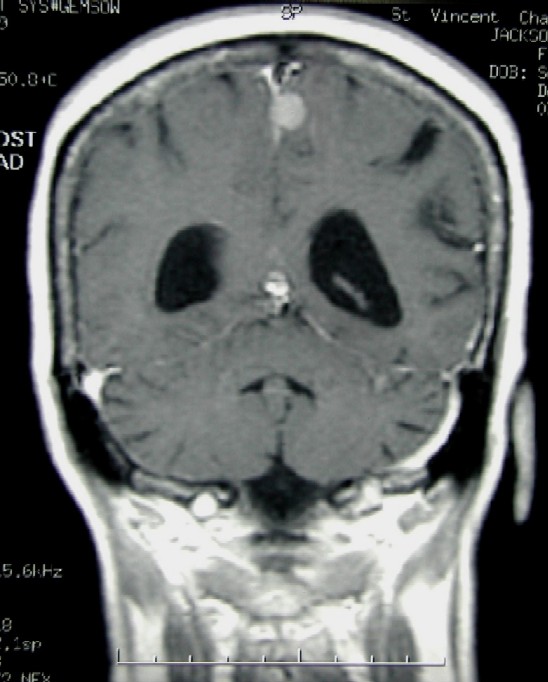
9- Coronal post-contrast
T1 spin echo (SE)
Good
supplement to axial post-contrast scan.
Normal
Small falx menengioma is clearly
seen.
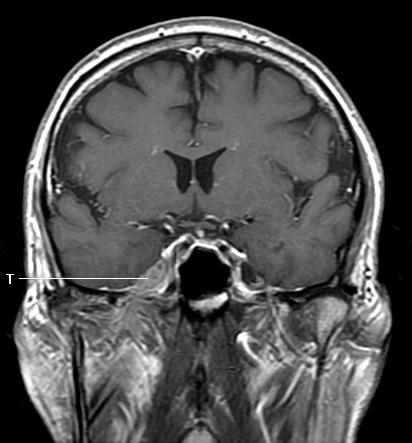
Perineural
spread of skin cancer to 5th nerve (T). Normal Meckel's Cave (cavum
trigeminale) seen on the contralateral side.